
Why Breast Cancer Survivors Need Heart-Healthy Eating: Research Update
The connections of breast cancer and heart disease are usually not what breast cancer survivors expect to discuss when they talk with a dietitian about breast cancer nutrition. Yet cardio-oncology nutrition research shows how heart-healthy eating choices can reduce influences on cardiovascular disease risk that often develop or worsen after a breast cancer diagnosis.
Want continuing education credit on this topic? Check here for my 3.5 CPEU course.
You’ll even get access to a bonus dietitian cheat sheet and a bonus handout you can use in your practice.
What You'll Find Here
♦ Research Now: Breast Cancer Survivors Face Cardiovascular Disease Risk?
♦ Why Breast Cancer Is Connected to Heart Disease
♦ High Blood Pressure and Breast Cancer: What’s the Connection?
♦ Metabolic Syndrome and Breast Cancer: A Powerful and Persistent Risk
♦ Smart Steps for Breast Cancer Survivors to Protect Heart Health
Breast cancer statistics show good news
… and a cautionary note
The good news is that women diagnosed with breast cancer now live longer than ever. Breast cancer death rates in the United States dropped 40% between 1989 and 2017.
- Today, more than 3.8 million women in the U.S. are living with or beyond breast cancer. That’s thanks to advances in early diagnosis, targeted treatments, and supportive care.
- 5-year survival rates are now 91%. And for most women facing breast cancer, they’re even better: Rates for localized breast cancer are 99%, and for regional cancer (which means there’s been spread to regional lymph nodes) they’re 86%.
- Average 10-year survival rate is 84%, and 15-year survival is now 80%.
The cautionary note:
Although women today are cured or living longer with breast cancer, current evidence shows that breast cancer survivors are at an increased risk for developing and dying from cardiovascular disease.
Research Now: Breast Cancer Survivors Face Cardiovascular Disease Risk?
For many women who’ve experienced a diagnosis of breast cancer, that becomes the focus when they think about their health.
But mounting research shows that women who have had breast cancer face increased risk of cardiovascular disease (CVD). In fact, several studies show that women with early-stage breast cancer are more likely to die from cardiovascular disease than from breast cancer.
- CVD was more common among breast cancer survivors than among women of similar age who had not had cancer in a massive study within a major cancer registry.
- CVD was more common even after statistically adjusting for age, race/ethnicity, risk factors, overweight or obesity, and smoking history.
- The study included only those who had survived at least 2 years after cancer diagnosis and everyone in the study was age 40 or older at cancer diagnosis.
- Cancer survivors were more likely to have CVD risk factors (such as hypertension, diabetes, and abnormal blood lipids) than people the same age without a cancer history.
- Breast cancer survivors were 65% more likely to die from cardiovascular disease than age-matched women who never had cancer in the CLUE II prospective cohort study.
- The greater rates of CVD deaths began 8 years after cancer diagnosis. Previous studies have similarly found increases beginning at about 7 years after diagnosis of breast cancer.
- Women older at cancer diagnosis showed a particular increase in CVD. Women ranged from age 45 to 84 at the beginning of the study. Among those age 70 and older at diagnosis, cancer survivors had more than double the CVD deaths as women the same age who never had cancer.
The call: grab hold of this “window of opportunity” from the time of breast cancer diagnosis through the years immediately following. A Scientific Statement from the American Heart Association – and conclusions of multiple researchers in cardio-oncology – highlight the need to use this time for early recognition and treatment of CVD risk factors.
Does Heart-Healthy Eating Matter for a Breast Cancer Survivor?
What would that even look like?
We’ll circle back to this important question!
Why Breast Cancer Is Connected to Heart Disease
The studies showing a greater toll of CVD among women living with and beyond breast cancer are observational studies. They can’t prove the cause of this association. Researchers in cardio-oncology report multiple potential reasons that heart health may be compromised.
Some Breast Cancer Treatments Can Damage the Heart and Blood Vessels
Radiation therapy to the left side of the chest wall may result in cardiomyopathy, damage to heart valves, and coronary heart disease (CHD). In the large blood vessels of the heart, radiation therapy causes inflammation and oxidative damage, which, especially in the presence of high cholesterol, leads to accelerated atherosclerosis. Radiation-related coronary atherosclerosis can develop within a few years after exposure or as a late-effect up to 20 or 30 years after treatment.
Some types of chemotherapy used for breast cancer can have cardiotoxic effects. Anthracyclines (e.g., doxorubicin, epirubicin), alkylating agents (e.g., cisplatin, cyclophosphamide), taxanes (e.g., paclitaxel), and antimetabolites (e.g., 5-fluorouracil, capecitabine) can each result in some harmful cardiovascular effects. These can include heart failure, myocarditis, thrombosis, and arrhythmias.
Some of the targeted therapies, like HER2 inhibitors (such as trastuzumab) and VEGF inhibitors — which have led to so much progress in treating breast cancer — markedly increase risk of hypertension and heart failure.
Aromatase inhibitors (AI) are a hormonal therapy for estrogen receptor-positive (ER+) cancer that’s especially used in postmenopausal women. Compared to women receiving tamoxifen as hormonal therapy, AI are linked with higher rates of hypertension, elevated LDL-cholesterol, and ischemic cardiovascular disease in some large clinical studies. However, researchers note that AI-related risks are not clear-cut, since many of the comparisons studied might show more about cardiovascular-protective effects of tamoxifen than about risk from the AIs themselves. Research continues.
Among women in the PATHWAYS study, compared to women without breast cancer who were of a similar age, race, and ethnicity, women with breast cancer had greater incidence of heart failure, CVD events (including stroke, arrhythmia, and cardiac arrest), and cardiovascular-related death.
- Over follow-up of 7 years on average, depending on treatment type, these risks ranged from a 26% increase to more than a 3-fold increase in risk
- Researchers are highlighting the study as another demonstration that women who are breast cancer survivors need ongoing monitoring and follow-up care for cardiovascular health.
Managing heart health risk factors is a key step after breast cancer.
Together, a woman and her healthcare team can go a long way protecting cardiovascular health.
Cardiovascular Risk Factors: Common in Women with Breast Cancer
A major focus in cardio-oncology has been CVD risk from toxicities of chemotherapy or radiation therapy. However, an analysis of data from women with breast cancer in the SEER database – with data from 18 cancer registries in the U.S. – suggests that monitoring cardiovascular health needs to extend wider. CVD risk in breast cancer patients who did not receive chemo- or radiation therapy was more than double that of women in the general U.S. population.
Major CVD risk factors include:
- Older age: Risk of breast cancer also increases with age up until age 80
- Smoking: Although smoking most strongly increases risk of CVD and lung cancer, it also raises risk of breast cancer.
- Diabetes: Type 2 diabetes is associated with greater risk of breast cancer. Many of the metabolic abnormalities in diabetes that pose cardiovascular risk also promote cancer development.
- Hypertension: A major influence on cardiovascular risk, it is also common in women with breast cancer. In breast cancer, it may develop as a side-effect of treatment. Or it may be present before breast cancer, since several factors that lead to elevated blood pressure also increased risk of breast cancer. More on this below
- Low physical activity: Common for many reasons, it leads to poor cardiovascular fitness and increases likelihood of developing other CVD risk factors. Regular physical activity reduces risk of breast cancer. Women with breast cancer may have already had low activity levels before their cancer diagnosis, or may have reduced activity as a result of joint pain or fatigue from cancer treatment, or both.
- Obesity: Excess body fat, especially visceral fat deep in the abdomen, promotes inflammation and oxidative stress, increasing both CVD and cancer risk. It also promotes insulin resistance (connecting it to Type 2 diabetes and breast cancer risk). And among postmenopausal women, it raises estrogen levels, which promotes estrogen-sensitive cancers like the most common form of breast cancer.
Some heart disease risk factors overlap as risk factors for breast cancer. And some CVD risk factors may increase because of cancer or its treatment.
Don’t ignore heart health after a breast cancer diagnosis.
Who is at greatest risk from a treatment that’s been identified with potential cardiotoxicity?
Current research says it’s those who:
✔ Were previously exposed to therapies that can have cardiovascular late effects (for example, during childhood, adolescent or young adult cancer)
✔ Have had a heart attack or have existing CVD
✔ Have 2 or more major CVD risk factors (smoking, hypertension, diabetes, dyslipidemia, obesity)
✔ Are age 60 or older
High Blood Pressure and Breast Cancer: What’s the Connection?

High blood pressure is a serious side effect of some cancer treatments that can occur quickly or many years later.
Hypertension is a major established risk factor for CVD. It causes structural changes in blood vessels and the heart that can lead to heart failure. And it’s one of the most frequent vascular toxicities of cancer treatment.
More than 40% of US women have hypertension. So, it’s not surprising if a woman has hypertension even before a diagnosis of breast cancer. Most Americans with hypertension do not have it under control, however.
High blood pressure is especially common in women with breast cancer.
- Hypertension is associated with greater risk of developing breast cancer. This increased risk (at least after menopause) may reflect risk factors like low physical activity, smoking, and excess body fat that increase risk of both high blood pressure and breast cancer. Risk of both increases with age. And some evidence suggests that hypertension itself might enhance development of breast cancer through increases in oxidative stress, increases in a vasoconstrictor hormone that lead to changes in growth factors, or other mechanisms, with more research needed.
- Some forms of breast cancer treatment can raise blood pressure. Some examples include VEGF inhibitors (which prevent formation of new blood vessels to slow growth and spread of tumors), platinum-based therapy (such as cisplatin), and HER2-targeted therapy (such as trastuzumab). Hypertension, especially when it’s poorly controlled, increases the risk of heart damage from chemotherapy. When blood pressure increases too much, it requires a pause or reduced dose in chemotherapy.
Sometimes hypertension develops or worsens rapidly during cancer treatment. And this may be temporary.
Hypertension can also occur as a late effect many years after cancer treatment. A normal blood pressure today does not mean a woman is “safe” from hypertension.
◊ ◊ ◊ ◊ ◊ ◊ ◊
To learn about choices within a plant-focused diet for better blood pressure, check here:
What Foods Help Lower Blood Pressure? Navigating the Research
◊ ◊ ◊ ◊ ◊ ◊ ◊
Metabolic Syndrome and Breast Cancer: A Powerful and Persistent Risk
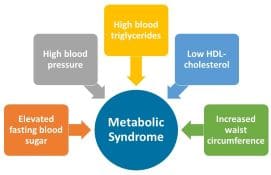
Presence of at least three of these five risk factors identifies metabolic syndrome.
Metabolic syndrome increases risk of CVD more than two-fold – and it increases risk of Type 2 diabetes more than four-fold. What you may not have heard is that metabolic syndrome also increases risk of several forms of cancer.
Metabolic syndrome is defined as abnormal levels or pharmaceutical treatment of three or more of the following: blood sugar, blood pressure, triglycerides, HDL cholesterol and waist circumference. Specific criteria differ in waist-size cut-points, but are otherwise similar in US and international scientific statements.
Metabolic syndrome is common in women with breast cancer:
- It’s common in US adults. About 1 in 3 US adults – and about half of women age 60 and older – have metabolic syndrome. Because it’s so common, many women with breast cancer already have metabolic syndrome when cancer is diagnosed.
- Metabolic syndrome is associated with greater risk of breast cancer among postmenopausal women. Although it’s unrelated to premenopausal breast cancer risk, it about doubles risk of postmenopausal breast cancer. Analysis shows that no single component (such as high blood pressure or high triglycerides) increases risk nearly as much as presence of the whole cluster of risk factors.
- This increased cancer risk probably reflects the effects of increased inflammation – both systemic and local in the breast micro-environment – and the effects of insulin resistance and elevated insulin levels. Since metabolic syndrome is strongly related to excess visceral fat, the increased levels of estrogen that occur in postmenopausal women with high body fat also likely add to breast cancer risk.
- Some forms of breast cancer treatment can promote metabolic syndrome – in both pre- and postmenopausal women. Certain types of chemotherapy and a targeted therapy that blocks a signaling pathway involved in cancer cell growth can increase development of metabolic syndrome. This can include increased insulin resistance with rise in blood sugar and elevated triglyceride levels, as well as increased LDL-cholesterol. And, as noted above, several types of chemotherapy can cause increases in blood pressure.
- Analysis in the PATHWAYS study shows how quickly metabolic syndrome can develop. The study included pre- and post-menopausal women diagnosed with stages I to III breast cancer who received chemotherapy either before (neoadjuvant therapy) or after (adjuvant therapy) surgery. Metabolic syndrome newly developed in 72.5% of these women within about four months during chemotherapy.
- In follow-up analysis to this study 4 to 5 years after chemotherapy ended, all components of metabolic syndrome had worsened beyond levels right after treatment. In addition, LDL-cholesterol and markers of insulin resistance and inflammation rose further. And weight, waist size, and % body fat all increased further, too.
For women with breast cancer who already have metabolic syndrome, or who develop it during treatment, greater number of metabolic syndrome components is associated with poorer outcomes.
Smart Steps for Breast Cancer Survivors to Protect Heart Health
Healthcare providers have cardio-oncology guidelines from major organizations for checking blood pressure and indicators of cardiovascular health before cancer treatment starts and for monitoring throughout treatment. Since hypertension can develop as a late effect many years after treatment, it’s vital that blood pressure – and other aspects of cardiovascular health – continue to be checked regularly.
Women living with and beyond breast cancer – especially those who have received a cancer treatment that can increase CVD risk – can make lifestyle choices to reduce development of hypertension and metabolic syndrome.
- Step one: limit sodium (just as is recommended for people who have not had cancer). The rise in blood pressure related to these cancer treatments appears to be sodium-sensitive, since it often involves sodium retention. For most people, the major sources of sodium come from highly processed foods. So don’t count on skipping the saltshaker as the solution. In overall research (not people with cancer), for those who have high sodium intake and hypertension, each drop in daily sodium of 1000 mg can reduce systolic blood pressure about 3 points (mm Hg).
- Check here to find doable tweaks for cutting sodium.
- Step back and look at overall eating habits, too. Research involving people who did not have cancer shows that a DASH-style diet can powerfully reduce risk of or help control high blood pressure. And the higher your blood pressure, or the more trouble you have limiting sodium, the greater its effectiveness. There’s no single “magic bullet” food for a healthy blood pressure. Benefits most likely come from how potassium, magnesium, nitrates and polyphenol phytochemicals, dietary fiber, and more act together to promote blood vessel health.
- Find out more about the ins and outs of a DASH diet here. You’ll see options to tweak it to include elements of Mediterranean-style eating habits if you want.
- Choose water as your go-to beverage. Coffee and tea can be great choices, too, if caffeine is kept within reason. The point is to limit sugar-sweetened beverages to no more than occasional use. Their concentrated calories promote weight gain. Moreover, frequent consumption is associated with increases in all the components of metabolic syndrome. And frequent consumption promotes higher circulating insulin levels and insulin resistance, major underlying mechanisms in metabolic syndrome.
- Look for small steps to avoid or limit weight gain. Excess body fat, especially excess visceral fat, is strongly linked to all the components of metabolic syndrome, including high blood pressure. It’s vital to avoid weight reduction efforts that result in loss of lean muscle mass. But even if weight gain can’t be completely avoided, finding small tweaks in eating and activity to limit it to modest amounts can help control blood pressure and metabolic health. And keeping weight gain to no more than 10% is associated with improved breast cancer related outcomes.
- Add walking or other movement. It’s important to get individualized advice from healthcare providers, since cancer or its treatment can make certain forms, amount, or intensity of exercise most safe.
- Overall research shows that regular moderate activity like walking can reduce systolic blood pressure about 5 mm Hg in people with hypertension. Moderate activity the equivalent of 30 minutes (not necessarily all at once) 5 times a week are less likely to develop metabolic syndrome. And getting more than that reduces risk even further. After physical activity, insulin sensitivity remains improved for 24 to 48 hours. So, finding a way to be active at least every other day can go a long way.
- For example, in a controlled intervention trial of women who completed breast cancer treatment within the last 6 months, supervised aerobic and resistance exercise three times per week for 16 weeks, the number of women with metabolic syndrome dropped from 77% to 15% of participants. All components of metabolic syndrome were reduced. And so were insulin resistance and biomarkers of inflammation.
- And as long as it’s approved by a woman’s healthcare provider, expert panels conclude appropriate physical activity can help cancer survivors reduce fatigue and improve health-related quality of life.
◊ ◊ ◊ ◊ ◊ ◊ ◊
Want an educational handout and dietitian cheat sheet that will help you clarify key strategies and address common questions about the cancer-CVD intersection?
These are two free bonuses with my 3.5 CPEU continuing education course for dietitians,
Cardiovascular Nutrition Across Cancer Treatment and Beyond:
Translating Evidence into Practice
.
Get CPE credit for deepening your understanding of the research in this area, with content not included in this website research review about building dietary patterns that promote cardiovascular health and cancer-related outcomes and providing extra attention to individualizing advice.
Get more information here about continuing education for dietitians.
◊ ◊ ◊ ◊ ◊ ◊ ◊
Here’s a Big Picture View of Cardio-Oncology Nutrition
A large study in the UK followed adults ages 40 to 70 who started off with no CVD or diabetes for up to 15 years. A healthy lifestyle score that included no current smoking, regular physical activity, a healthy diet, no more than moderate alcohol consumption, and adequate sleep. (A diet was considered healthy if it met recommendations for at least 4 of these: adequate amounts of fruits, vegetables, whole grains, and fish; and limited refined grains, red meat, and processed meat.)
- Among all the people in the study who had been diagnosed with cancer, compared to people with low scores, those with highest scores for a healthy lifestyle were nearly half as likely to develop CVD in the years ahead.
- Among women who had been diagnosed with breast cancer, each 1-point increase in healthy lifestyle score was associated with a 20% lower risk of developing CVD.
Bottom Line on Heart-Healthy Eating for Breast Cancer Survivors
The journey is different for each individual person living with and beyond breast cancer. And priorities for nutrition and other lifestyle choices can change over time. Diagnostic and treatment advances have brought such improvements in breast cancer outcomes that breast cancer survivors now need to consider heart health in their lifestyle choices.
Fortunately, choices that support positive breast cancer outcomes have room to include choices that reduce risk of cancer in the future and promote heart health.
Sign up: If you aren’t already receiving my research reviews by email, sign up so you won’t miss any of the fascinating topics coming in future reviews! Just click here.
Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009 Oct 20;120(16):1640-5.
American Cancer Society. Breast Cancer Facts & Figures 2019-2020. Atlanta: American Cancer Society, Inc. 2019.
Armenian SH, Lacchetti C, Barac A, et al. Prevention and Monitoring of Cardiac Dysfunction in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2017 Mar 10;35(8):893-911.
Armenian SH, Xu L, Ky B, et al. Cardiovascular Disease Among Survivors of Adult-Onset Cancer: A Community-Based Retrospective Cohort Study. J Clin Oncol. 2016 Apr 1;34(10):1122-30.
Campbell KL, Winters-Stone KM, Wiskemann J, et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Medicine & Science in Sports & Exercise. 2019;51(11), 2375-2390.
Cao Z, Xu C, Yang H, Li S, Wang Y. The Role of Healthy Lifestyle in Cancer Incidence and Temporal Transitions to Cardiometabolic Disease. JACC CardioOncol. 2021 Dec 21;3(5):663-674.
Centers for Disease Control and Prevention. Hypertension Cascade: Hypertension Prevalence, Treatment and Control Estimates Among U.S. Adults Aged 18 Years and Older Applying the Criteria from the American College of Cardiology and American Heart Association’s 2017 Hypertension Guideline—NHANES 2015–2018. Atlanta, GA: U.S. Department of Health and Human Services; 2021.
Curigliano G, Lenihan D, Fradley M, et al. Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations. Ann Oncol. 2020 Feb;31(2):171-190.
Dieli-Conwright CM, Courneya KS, Demark-Wahnefried W, et al. Effects of aerobic and resistance exercise on metabolic syndrome, sarcopenic obesity, and circulating biomarkers in overweight or obese survivors of breast cancer: a randomized controlled trial. J Clin Oncol. 2018;36(9):875-883.
Dieli-Conwright CM, Wong L, Waliany S, et al. An observational study to examine changes in metabolic syndrome components in patients with breast cancer receiving neoadjuvant or adjuvant chemotherapy. Cancer. 2016 Sep 1;122(17):2646-53.
Dieli-Conwright CM, Wong L, Waliany S, Mortimer JE. Metabolic syndrome and breast cancer survivors: a follow-up analysis after completion of chemotherapy. Diabetol Metab Syndr. 2022 Mar 3;14(1):36.
Demark-Wahnefried W, Schmitz KH, Alfano CM, et al. Weight management and physical activity throughout the cancer care continuum. CA Cancer J Clin. 2018 Jan;68(1):64-89. doi:10.3322/caac.21441
Greenlee H, Iribarren C, Rana JS, et al. Risk of Cardiovascular Disease in Women With and Without Breast Cancer: The Pathways Heart Study. J Clin Oncol. 2022 Apr 6:JCO2101736.
Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005; 112: 2735–2752.
Guan T, Zhang H, Yang J, et al. Increased Risk of Cardiovascular Death in Breast Cancer Patients Without Chemotherapy or (and) Radiotherapy: A Large Population-Based Study. Front Oncol. 2021 Jan 28;10:619622.
Herrmann J. Adverse cardiac effects of cancer therapies: cardiotoxicity and arrhythmia. Nat Rev Cardiol. 2020 Aug;17(8):474-502.
Jung AY, Hüsing A, Behrens S, et al. Postdiagnosis weight change is associated with poorer survival in breast cancer survivors: A prospective population-based patient cohort study. Int J Cancer. 2021 Jan 1;148(1):18-27.
Li, P., Wang, T., Zeng, C. et al. Association between metabolic syndrome and prognosis of breast cancer: a meta-analysis of follow-up studies. Diabetol Metab Syndr. 2020;12:10.
Malik VS, Hu FB. Sugar-Sweetened Beverages and Cardiometabolic Health: An Update of the Evidence. Nutrients. 2019 Aug 8;11(8):1840.
Mehta LS, Watson KE, Barac A, et al. Cardiovascular Disease and Breast Cancer: Where These Entities Intersect: A Scientific Statement From the American Heart Association. Circulation. 2018 Feb 20;137(8):e30-e66.
Micucci C, Valli D, Matacchione G, Catalano A. Current perspectives between metabolic syndrome and cancer. Oncotarget. 2016 Jun 21;7(25):38959-38972.
Mohammed T, Singh M, Tiu JG, Kim AS. Etiology and management of hypertension in patients with cancer. Cardiooncology. 2021 Apr 6;7(1):14.
Okwuosa TM, Morgans A, Rhee JW, et al. Impact of Hormonal Therapies for Treatment of Hormone-Dependent Cancers (Breast and Prostate) on the Cardiovascular System: Effects and Modifications: A Scientific Statement From the American Heart Association. Circ Genom Precis Med. 2021 Jun;14(3):e000082.
Ramin C, Schaeffer ML, Zheng Z, et al. All-cause and cardiovascular disease mortality among breast cancer survivors in CLUE II, a long-standing community based cohort. J Natl Cancer Inst. 2021;113(2):137–145.
Virani SS et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation. 2020 Mar 3;141(9):e139-e596.
Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. Hypertension. 2018 Jun;71(6):e13-e115.
World Cancer Research Fund/American Institute for Cancer Research.
Diet, Nutrition, Physical Activity and Cancer: A Global Perspective.
Continuous Update Project Expert Report, 2018. [The AICR Third Expert Report] Available at: aicr.org/research/third-expert-report/
Zhang D, Liu X, Liu Y, et al. Leisure-time physical activity and incident metabolic syndrome: a systematic review and dose-response meta-analysis of cohort studies. Metabolism. 2017;75:36-44.
Zhao P, Xia N, Zhang H, Deng T. The Metabolic Syndrome Is a Risk Factor for Breast Cancer: A Systematic Review and Meta-Analysis. Obes Facts. 2020;13(4):384-396.
2 Comments
Leave a Comment
Published : May 16, 2022 | Last Updated: September 2, 2025
Tagged: breast cancer, breast cancer survivors, cardio-oncology, cardiovascular disease, CVD, heart health, high blood pressure, hypertension
Meet the author/educator

Karen Collins
MS, RDN, CDN, FAND
I Take Nutrition Science From Daunting to Doable.™
As a registered dietitian nutritionist, one of the most frequent complaints I hear from people — including health professionals — is that they are overwhelmed by the volume of sometimes-conflicting nutrition information.
I believe that when you turn nutrition from daunting to doable, you can transform people's lives.
Accurately translating nutrition science takes training, time and practice. Dietitians have the essential training and knowledge, but there’s only so much time in a day. I delight in helping them conquer “nutrition overwhelm” so they can feel capable and confident as they help others thrive.
I'm a speaker, writer, and nutrition consultant ... and I welcome you to share or comment on posts as part of this community!
{kind=link}
Karen, thank you so much for this excellent article on breast cancer and heart disease. I appreciate that you also provided us with simple/practical ways breast cancer survivors can protect their heart health. It would also be helpful to get more resources about nutrition and breast cancer (based on cancer’s genes or hormones). I often get a referral from MDs with patients wanting to know more about the best nutrition approach for their specific breast cancer type. I usually provide them with Oncology Academy DPG resources, but it is general information. I feel I am not fully supporting my patients even after discussing low-fat/soy/alcohol, etc. Am I missing any critical data/resources I should be discussing with breast CA patients? Are there any reputable resources that offer doable/nutrition guidelines for a patient with specific breast cancer types. Thank you, and I greatly appreciate your expertise.
Shea
Thank you for the positive feedback on this article, Shea. I’m glad it’s helpful to you.
Regarding resources about specific nutrition guidelines based on subtypes of breast cancer, I am not aware of any evidence strong enough at this time to support such an approach. My understanding is that priorities may differ at different stages of the cancer journey (immediately after surgery, during active chemo, following treatment, etc.) and based on different health conditions that may exist or develop (such as diabetes or high blood pressure). Beyond this, researchers may have hypotheses they are testing about different responses to diet. But we still have so much to learn about diet during breast cancer treatment, that it’s my understanding that we are still some time away from being able to define dietary specifics based on cancer subtype or individual genetic tendencies.
It can be frustrating for people with cancer when they see media headlines suggesting possibilities based on lab research or single studies, but we need to support them in taking basic well-supported steps without jumping to make changes prematurely based on very tentative evidence.