

Latest Hypertension Guidelines: Key Nutrition Insights
Inside: Get clear, practical insights on the nutrition and lifestyle recommendations in the AHA’s latest hypertension guidelines, including how to tailor them.
When a problem is so common that many of the people you know also experience it, that can make it easy to downplay the importance of addressing it.
A prime example: Hypertension.
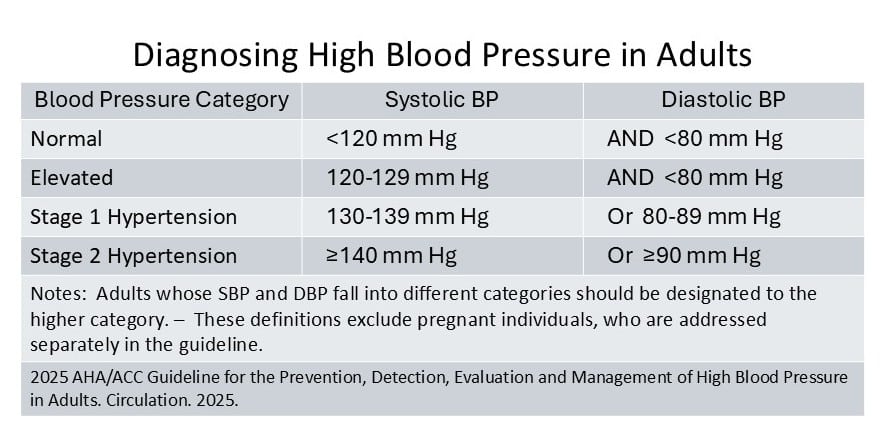
Based on current guidelines on diagnosis and treatment of high blood pressure, 46.7% of U.S. adults now have hypertension (defined as blood pressure ≥130/80 mm Hg or receiving antihypertensive therapy).
High blood pressure is the most common modifiable risk factor for cardiovascular diseases – that includes coronary artery disease, heart failure, atrial fibrillation, stroke, dementia, and chronic kidney disease.
Yet dietitians can often find themselves working with people who overlook:
- Blood pressure’s significance to health,
- The successful control that’s possible today,
- And – perhaps most common – the impact that a few adjustments in nutrition and lifestyle could have.
KEY TAKE-AWAY POINTS
♦ Risks of high blood pressure begin early, and this research is the basis for several updates in the latest AHA/ACC hypertension guideline.
♦ Nine nutrition and lifestyle interventions are recommended for people with or without hypertension, regardless of whether or not they also receive medications for blood pressure control.
♦ Potassium-based salt substitutes are one of the strategies suggested, but there are several considerations related to their use.
♦ DASH diet nutrition research continues, with important findings related to prevention of hypertension, reduced need for hypertensive medications, and benefits even for treatment-resistant hypertension.
♦ Nutrition strategies for blood pressure management can include a broad range of factors, including potassium-rich foods, plant-forward dietary patterns and types of dietary fiber… and attention to factors that could be raising blood pressure.
Hypertension Guidelines Highlight: Risk Begins Early
The guidelines recommend that all adults should aim for blood pressure (BP) <130/80 mm Hg, with <120/80 (normal blood pressure) even better if it’s attainable.
High blood pressure is only to be diagnosed based on an average of at least two measurements taken at least a minute apart on at least two occasions. And blood pressure needs to be measured carefully, watching for factors like time at rest, talking, caffeine and exercise before and during measurement. (See details in the guideline: Figure 3 for office measurement and Figure 4 for home BP measurement.)
Reasons for Blood Pressure Control Are Growing
- Cognitive decline and dementia: There is stronger proof now that high blood pressure increases risk.
- Chronic kidney disease: High blood pressure is identified as the most common modifiable risk factor.
- Stroke, coronary artery disease, and heart failure: Hypertension has long been known as the leading modifiable risk factor, and the higher the blood pressure, the greater the risk.
Prevention is Best
As blood pressure rises above normal (SBP ≥120 mm Hg and DBP ≥80 mm Hg), vascular damage can begin that is irreversible, increasing cardiovascular disease risk.
Treating hypertension is vital to reduce CVD risk.
But even if treatment reduces blood pressure to <120/80, those individuals still have twice the risk of CVD compared to adults without hypertension who maintain blood pressure <120/80 without treatment.
The AHA/ACC guidelines say that this highlights the importance of primary prevention of blood pressure elevation.
Lower is Better
Each increase in blood pressure is associated with further increase in CVD risk, according to observational studies that follow people over time. And in controlled clinical trials involving adults at high risk for CVD, more intensive treatment to reach a lower blood pressure target is more effective for preventing CVD.
Strong evidence supports a goal of keeping systolic blood pressure <130 mm Hg. Some evidence supports even greater potential benefit from a systolic blood pressure <120 mm Hg, but data is more limited and if intensive antihypertensive therapy is needed to reach that level, potential adverse effects need to be considered.
Blood Pressure Treatment Thresholds: New Procedure
“Risk-based treatment” is an essential focus of the guidelines, spelled out as being based on a new risk calculator. For people with blood pressure of 120-129/<80, lifestyle is the recommended therapy; not medication. For those with blood pressure of 130-139 systolic or 80-89 diastolic, medications are to be added based on CVD risk.
The PREVENT™ risk calculator replaces Pooled Cohort Equations for determining when to initiate medication in patients without clinical CVD.
- PREVENT expands beyond previous ASCVD-focused models with options for including kidney function, metabolic measurements, and neighborhood deprivation index.
- The PREVENT equations can be included in electronic health records to support shared decision-making and personalized care across broad populations and care settings.
When to Initiate BP Medications: Based on Context of Overall CVD Risk
The guideline attempts to walk the line between recognizing that since CVD risk begins at even Stage 1 hypertension it makes sense to avoid delay in reaching a healthier level, while also avoiding unnecessary medication and giving the benefits of lifestyle change a chance.
Begin antihypertensive medical therapy if:
- BP ≥140/90 mm Hg, regardless of risk.
- BP ≥130/80 mm Hg and:
- Clinical cardiovascular disease, chronic kidney disease, or diabetes
- 10-year CVD risk ≥7.5% (per the PREVENT calculator)
- BP ≥130/80 mm Hg with risk <7.5%: Initiate medications only if average systolic BP remains ≥130 mm Hg or average diastolic BP remains ≥80 mm Hg after 3–6 months of lifestyle therapy.
The overarching blood pressure treatment goal is <130/80 mm Hg for all adults, with additional considerations for those who require institutional care, have a limited predicted lifespan, or are pregnant.
If blood pressure is “a little high”, finding doable steps for a healthier lifestyle is job #1.
Hypertension Guidelines: Nutrition and Lifestyle Strategies Are for Everybody
 Lifestyle change remains first-line therapy and is recommended for all adults, with or without hypertension.
Lifestyle change remains first-line therapy and is recommended for all adults, with or without hypertension.
- Use lifestyle approaches as sole therapy in lower-risk adults or as adjuncts when medications are needed.
- Test effects of lifestyle before medication for lower-risk adults (PREVENT risk <7.5%) with SBP ≥130 or DBP ≥80: Lifestyle changes should be trialed and sustained for 3–6 months before initiating medications.
For people with or without hypertension, regardless of whether or not they also receive medications for blood pressure control, the 2025 AHA/ACC guideline recommends nine lifestyle interventions.
Eat DASH style:
A diet rich in fruits, vegetables and whole grains; with low-fat dairy and other lean protein sources, dried beans, nuts and healthy oils (with limited saturated fat and sweets).
– In a previous research brief, we explored some simple swaps you can show people to DASH-ify their eating habits for better blood pressure.
🏆 Expected systolic BP reduction: 5-8 mm Hg with hypertension (hpt) – 3-7 mm Hg without hpt
Limit sodium:
Consume <2300 mg/day. The AHA guideline advises working toward 1500 mg/day as the ideal.
– People vary in how their BP responds. Older adults and people with higher BP that is salt-sensitive respond with greater BP reduction.
– Good news: A target of 1500 mg/day may not be realistic for many people. But even cutting 1000-1200 mg/day can reduce blood pressure. – A meta-analysis of 133 randomized trials found that each 1150 mg reduction in 24-hour urinary sodium (the most reliable marker of sodium consumption) reduced systolic BP by 1.10 mm Hg and diastolic BP by 0.33 mm Hg. – And trials that lasted more than 14 days found systolic BP reduction double that overall average.
– Guide people to look beyond the salt shaker and focus on swapping out their most frequent high-sodium processed food choices. With a few doable tweaks, sodium can be reduced by 1000 mg (or more).
– For people with severe, symptomatic orthostatic hypotension, sodium reduction may be contraindicated, the guideline notes.
🏆 Expected systolic BP reduction: 6-8 mm Hg with hpt – 1-4 mm Hg without hpt
Choose more potassium-rich foods:
Potassium consumption lowers blood pressure by direct effect on vascular tone and by stimulating urinary excretion of excess sodium. The AHA guideline advises aiming for 3500 to 5000 mg of potassium per day, especially for people with elevated blood pressure or hypertension.
– Encourage foods with more potassium among daily choices. But note: the DASH diet recommended in point #1 is already designed to increase dietary potassium by boosting consumption of vegetables, fruits, and legumes and including low-fat dairy.
– The guideline notes that supplemental potassium could also be used for those with elevated BP or hypertension, although this would provide potassium without any of the other blood pressure-protective nutrients commonly found in high-potassium foods.
🏆 Expected systolic BP reduction: 6 mm Hg with hpt – 3-6 mm Hg without hpt
Consider a potassium-based salt substitute:
The guideline advises salt subs for dual benefits, reducing sodium and enhancing potassium intake.
– However, there are important factors to consider to evaluate the likelihood of benefits and make sure someone is not at risk because of chronic kidney disease or use of drugs that reduce potassium excretion. – See more details below.⬇️
🏆 Expected systolic BP reduction: 5-7 mm Hg with hpt – 5 mm Hg without hpt
Explore possibilities to drop a few pounds (for those with overweight or obesity):
The guideline recommends a sustained reduction of ≥5% in body weight, an amount that research generally supports as clinically meaningful for effects on blood pressure.
– Emphasize that it’s not necessary to reach what standard calculations identify as “ideal” weight. Instead, it’s more important to aim for a weight that an individual can maintain with realistic new habits.
🏆 Expected systolic BP reduction: about 1 mm Hg for each 2-pound weight loss (1 kg). – Achieving a sustained loss of ≥5% is identified as likely to reduce systolic BP about 6-8 mm Hg with hpt – 3-5 mm Hg without hpt
Limit alcohol:
Alcohol does not have a free pass when it comes to heart health, since too much raises blood pressure. The guidelines identify abstinence from alcohol as optimal for best health. For people whose drinking is beyond what’s classified as moderation, the guidelines call for reducing amounts by at least half, to a maximum of 2 drinks/day for men, 1 for women).
– For people who currently drink ≤2 drinks per day, the guidelines say that reducing intake further is unlikely to significantly lower blood pressure, although it can still be recommended for other health benefits.
– These recommendations define one standard drink as one that contains 14 grams of ethanol: 12 oz. beer, 5 oz. wine, 1½ oz. of 80-proof spirits.
🏆 Expected systolic BP reduction: 4-6 mm Hg with hpt – 3 mm Hg without hpt
Make room for movement:
Guidelines advise 90-150 minutes per week of aerobic physical activity and/or resistance training. Even taking a 30-minute brisk walk three to five days a week can significantly lower systolic blood pressure in people with and without hypertension.
– Blood pressure benefits aren’t all-or-nothing, and are reached with lower- and higher-intensity exercise, whether continuous or intermittent. Dose-response analysis shows an average 2/1 mm Hg reduction for each additional 30 minutes of aerobic exercise per week, with the largest BP reduction at 150 minutes per week.
🏆 Expected systolic BP reduction from 90-150 minutes/week of aerobic exercise: 4-8 mm Hg with hpt – 2-7 mm Hg without hpt – Blood pressure reduction from dynamic resistance (e.g., weight lifting) and isometric resistance exercise (e.g., hand grip) varies, but both offer significant benefits.
Incorporate stress management:
Two recommendations suggest tools that may be helpful to prevent or treat elevated blood pressure and hypertension. These recommendations are classified as weaker recommendations compared to the others, because the evidence base supporting them is only moderate.
– Transcendental meditation is one option that may be a reasonable choice, with two 20-minute sessions/day suggested.
– Other forms of stress management, such as breathing control techniques about 15 minutes/day) or yoga, are also identified as options that may be reasonable strategies for blood pressure management.
🏆 Expected systolic BP reduction: 5-7 mm Hg with hpt – 5 mm Hg without hpt
Important Notes on Use of Potassium-Based Salt Substitutes 

Caution is needed with potassium-based salt substitutes in some individuals:
- People with Chronic Kidney Disease (CKD)
- Those taking medications that reduce potassium excretion, including (but not limited to):
- Potassium-sparing diuretics (e.g., amiloride, triamterene)
- Mineralocorticoid receptor antagonists- also known as aldosterone antagonists (e.g., spironolactone, eplerenone, finerenone)
- Angiotensin-converting enzyme inhibitors – also known as ACE inhibitors (e.g., captopril, enalapril, lisinopril, benazepril, and others)
- Angiotensin receptor blockers – also known as ARBs (e.g., losartan, valsartan, candesartan, telmisartan, and others)
- Some immunosuppressive agents (e.g., cyclosporine, tacrolimus)
- Monitoring serum potassium is advised when combining potassium-rich diets or potassium-based salt substitutes with these medications.
All salt substitutes are not the same: The guideline refers to use of a salt substitute that is 25%-30% potassium chloride and 65%-75% sodium chloride, which is the type that has been used in many studies and tends to have a more acceptable, less bitter taste than products with a higher proportion of potassium.
- However, many of the most widely available salt substitutes are not simply “potassium-enriched salt”, they contain no NaCl at all, and are 100% KCl. Each ¼ teaspoon of these contains from 530 to 690 mg of potassium, the equivalent of eating an extra 1½ medium bananas.
- Salt substitutes used in research have varied from 25% to 65% potassium chloride (KCl), with 33% to 75% sodium chloride (NaCl). In a meta-analysis of 19 studies on salt substitutes and blood pressure, all products lowered systolic blood pressure comparably, though products with less than 65% NaCl lowered blood pressure a bit more.
- Especially with commonly available products that are 100% KCl, there’s reason for concern that medications that reduce potassium excretion may be added for blood pressure control at some point without inquiring about salt substitute use, posing risk of elevated blood potassium levels.
Worth considering: The report briefly notes that research showing the effectiveness of potassium-based salt substitutes comes largely from studies in which salt in cooking or at the table is people’s primary source of sodium, and thus may be of greatest benefit in those with similar sources of sodium intake.
- For the majority of Americans – whose excessive sodium intake comes from processed foods and foods prepared in restaurants – salt substitutes alone may bring limited ability to meet recommended dietary sodium levels.
- For people who add salt at the table and in cooking, a potassium-based salt substitute can further increase potassium intake beyond what is achieved through a DASH-style diet and attention to food choices high in potassium. – But it’s important to clarify: the increase in potassium may be beneficial, but unlike the changes in food choices, it is not providing the additional blood pressure-protective nutrients and compounds.
DASH Diet Nutrition Research: Important Context for Dietitians 

DASH Diet Reduces Risk of Developing Hypertension
People whose diets were most closely aligned with a DASH diet were nearly 20% less likely to develop hypertension than those whose diets were least aligned with the pattern in an analysis of nine observational studies that followed adults over time.
When analysis removed the prospective cohort studies that were of lower methodological quality, the remaining five higher quality prospective cohort studies showed this association quite consistently, providing the strongest evidence of this association.
DASH Diet Reduces Need for Blood Pressure Medications in People with Hypertension
The ENCORE study included 144 men and women with hypertension (BP 130–160/80–99 mm Hg) not being treated with medications who had overweight or obesity and a sedentary lifestyle but no heart disease, chronic kidney disease, or medication-treated diabetes.
- Participants were randomized to 16 weeks of DASH (Dietary Approaches to Stop Hypertension) diet plus behavioral weight management (DASH + WM), DASH diet alone (DASH), or Usual Care.
- They were classified as whether medical antihypertensive therapy was indicated based on recommendations of the previous (2017) ACC-AHA Hypertension Guideline. (Criteria for drug therapy included either BP ≥140/90 mm Hg — or BP ≥130/80 mm Hg in people with an estimated 10-year CVD risk ≥10% or a diagnosis of diabetes.) The decrease in CVD risk was due to both BP reduction and improved blood cholesterol.
Results:
- Blood pressure decreased by a mean of 16.1/9.9 mm Hg in DASH + WM and a mean of 11.2/7.5 mm Hg in DASH, whereas in Usual Care systolic BP did not change significantly and diastolic BP decreased 3.8 mm Hg.
- 10-year risk of a CV event decreased. After adjustment for baseline values, risk fell to 4.4% in the DASH + WM group and to 5.0% in the DASH group (both statistically significant changes), but did not significantly change in the Usual Care control group.
- Indication for BP-lowering drugs was reduced. Participants who would be appropriate for medication decreased from 51% to 18% of participants in the DASH + WM group and from 48% to 22% in the DASH group, but no significant change occurred in the Usual Care group.
This research thus suggests that nearly two-thirds of patients with modestly elevated BP who meet criteria for antihypertensive drug therapy can achieve BPs in the desired range with an intensive lifestyle modification program, avoiding the costs, inconvenience, and potential side effects of drug treatment.
Important note: People were not left on their own to follow the DASH or DASH + WM protocols. – The intervention involved 2 weeks with food provided, followed by 14 weeks of frequent support from registered dietitian nutritionists with individual counseling and small group education.
DASH Diet as Part of Lifestyle Intensive Intervention Can Reduce Even Resistant Hypertension
Treatment-resistant hypertension is blood pressure that remains above goal despite adherence to treatment with three or more optimally dosed antihypertensive medications of different classes, including a diuretic. Some people may think that means hypertension diet advice wouldn’t work for these people, but that’s not the case.
In the TRIUMPH study, participants with treatment-resistant hypertension were randomly assigned to a 4-month structured program provided within a cardiac rehab setting or a control group.
- In the intervention group, a registered dietitian nutritionist taught participants about a DASH diet reduced in calories and sodium (≤2300 mg/d). The well-rounded program also provided weekly group sessions designed to support long-term behavior change and aerobic exercise at a cardiac rehab facility three times a week.
- The control group of participants received a 1-hour educational session from a health educator about BP management along with a workbook that contained an individualized diet and exercise program with instruction on the same DASH diet with caloric restriction and exercise program as what was provided in the active intervention group.
Results:
Compared to participants who received only brief education and a workbook, those in the lifestyle intervention group:
- Clinic systolic BP decreased more (decreasing 12.5 mm Hg instead of 7.1 mm Hg)
- 24-hour ambulatory systolic BP decreased more (decreasing 7.0 mm Hg, with no reduction in the other group)
- Flow-mediated dilation, a measure of vascular endothelial function, tended to improve, whereas levels already categorized as impaired worsened further in the control group.
When the DASH diet is continued over time (beyond the four months of this intervention), its inclusion of foods for vascular health might help slow vascular aging in more ways. Further research is needed.
Blood Pressure in People During and After Cancer Treatment: One of the most common CVD risks
Want CPE credit for learning more about how nutrition for better blood pressure fits as part of cancer treatment and survivorship care?
💡 Check out my on-demand continuing education course:
Cardiovascular Nutrition Across Cancer Treatment and Beyond: Translating Evidence into Practice
This special CPE program designed for dietitians focuses on the intersection of cardiovascular and cancer nutrition.
🚀 You’ll gain 3.5 credits in one comprehensive, self-paced course — broken into shorter modules to fit your busy schedule.
Find out more here.
Nutrition for High Blood Pressure: Closer Look, Broader Picture

Increasing Potassium Consumption through Foods
The AHA guideline sets a goal of 3500-5000 mg of potassium per day.
Current intake in the US averages 2900 mg/day in adult men and 2300 mg/day in adult women.
- Fruits, vegetables, and legumes are major sources of potassium, and the recommended DASH diet will increase potassium consumption for most people. What’s more, focusing on the foods emphasized in this dietary pattern may act through multiple mechanisms to support a healthy blood pressure, because many of these foods are sources of magnesium, nitrates, and polyphenols, as well as dietary fiber. – People whose DASH-style diet includes fish and/or dairy products get a substantial boost to potassium from these foods, too.
- Want a resource to educate people about potassium sources? USDA MyPlate offers two versions: one showing potassium content in standard servings (e.g., 1 cup of vegetables and fruits, 3 oz. of seafood and meat) and a similar handout showing smaller portions (e.g., ½ cup of most vegetables and fruits, seafood and meat per ounce).
- Other foods provide potassium, too. Although they contain less potassium per serving than the foods listed on the MyPlate handout, whole grains, nuts, coffee, and tea all provide around 90 to 150 mg or more per serving. For many people these can be significant contributors to potassium intake.
Plant-forward Diets and Blood Pressure
Recommended dietary patterns might benefit blood pressure through effects on the gut microbiome.
An AHA Science Advisory reviewed research on effects of the gut microbiome on development of hypertension. The advisory noted potential for dietary influences on the microbiome-gut axis to benefit blood pressure. But it concludes that this is not yet supported by strong enough evidence to target microbiome-focused strategies at this time for blood pressure management.
On the other hand, focusing on a healthy dietary pattern that is supported by strong evidence for blood pressure control may bring benefits through mechanisms that include influence on the gut microbiome.
You’ll find more here to help address questions about “What foods help lower blood pressure?”
Fermentable Fiber: Is Better Blood Pressure One of Its Benefits?
Short-chain fatty acids (SCFA) produced in the colon from resistant starch and other fermentable fibers can activate receptors in the gut and kidneys that reduce BP and inflammation. – However, when those SCFAs are consumed orally, blood pressure has increased in some studies.
One meta-analysis of trials of adults with hypertension graded evidence as high certainty that increasing fiber consumption reduces systolic and diastolic blood pressure, by about 4 and 3 mm Hg, respectively.
- According to dose-response analysis, an increase of 5 grams of fiber per day reduces systolic BP about 2.8 mm Hg (range − 3.8 to − 1.8) and diastolic BP about 2.1 mm Hg (range − 3.0 to − 1.2).
- This improvement in pre-existing hypertension was seen in people with and without BP medications.
- This study notes that effects may be through several mechanisms, including effects of increased insulin sensitivity on endothelial function, as well as high-fiber foods providing antioxidants and nitrate that improve vasodilation and reduce oxidative stress. – So it’s not exclusively through the gut microbiome.
Check for Factors Raising Blood Pressure that Get Overlooked
The AHA guidelines flag several prescription and non-prescription drugs that may cause elevated blood pressure (complete list in Table 11 of the guideline).
Several choices that fall within topics dietitians discuss with people also warrant attention.
- Caffeine should be kept <300 mg/day for hypertension management, according to the AHA guidelines. And people with severe uncontrolled hypertension are advised to avoid >1 cup/day.
- Coffee and tea can be part of a blood pressure-friendly diet, however. Limited research links habitual consumption of 2-3 cups/day with lower risk of CVD mortality and either modestly lower risk of developing hypertension or no effect on blood pressure and hypertension risk.
- Ephedra (Ma Huang) and prolonged daily consumption of licorice have strong evidence for independently increasing blood pressure, regardless of drug interactions.
- St. John’s Wort does not typically raise blood pressure on its own but poses a significant hypertensive risk when combined with MAOIs, SSRIs, or certain other medications.
- Other herbs such as guarana, bitter orange, and yohimbine may also independently elevate blood pressure or do so through interactions. – It’s important to know about use of herbal supplements, especially in patients taking cardiovascular or psychotropic medications.
Want a free client-ready guide to help clients focus on their personal next steps?
Step by Step: Eating for a Healthy Blood Pressure
⇒ Explore a variety of foods that offer protective influences on blood pressure, as well as healthy swaps for hidden sources of excess sodium.…
⇒ Get the guide here.
Bottom Line on Nutrition and the Hypertension Guidelines:
The updated blood pressure guidelines are trying to clarify that “a little bit of high blood pressure” is not something to passively watch. The health risks of high blood pressure are too great to delay medical treatment when it’s needed.
On the other hand, nutrition remains a powerful first-line therapy for preventing and managing hypertension as part of a healthy lifestyle, bringing meaningful reductions in risk of heart attack, stroke, and cognitive decline. Ongoing research with the DASH diet provides a powerful support for what defines a blood pressure-protective dietary pattern.
For some people, diet won’t be enough. But if diet hasn’t “worked” to reduce blood pressure before, it is worth an effort to explore the full picture of tailoring dietary strategies like DASH, sodium reduction, potassium optimization, and weight reduction (with or without medical therapy for weight loss). Intervention trials showing benefits of successful dietary change tend to involve multiple sessions with a registered dietitian nutritionist to address barriers and move step-by-step into individualized eating habit changes.
If you found this update helpful, please share it!
I’d love it if you share this on social media or by email to a friend, family member, or colleague.
Sign up: If you aren’t already receiving my research reviews by email, sign up so you won’t miss any of the fascinating topics coming in future reviews! Just click here.
Step by Step: Eating for a Healthy Blood Pressure
- Client-ready guide to help you explore a variety of foods that offer protective influences on blood pressure, as well as healthy swaps for hidden sources of excess sodium.…
- ⇒ Get my free guide here.
Talking about the DASH diet
- Details about the diet and tips for success from the National Institutes of Health
- A free client-ready DASH diet handout from the National Lipid Association
Talking about increasing potassium consumption
- The National Institutes of Health Office of Dietary Supplements has a fact sheet in consumer and health professional versions that summarizes research on health, dietary intake, and groups of concern.
- USDA MyPlate offers two versions: one showing potassium content in standard servings (e.g., 1 cup of vegetables and fruits, 3 oz. of seafood and meat) and a similar handout showing smaller portions (e.g., ½ cup of most vegetables and fruits, seafood and meat per ounce).
Talking about accurately measuring blood pressure
- The American Heart Association provides, Top Things to Know: Measurement of Blood Pressure in Humans.
- Also from the AHA, How to Accurately Measure Blood Pressure at Home, has information about home blood pressure monitors and tips for accurate measurement.
- And here’s an AHA infographic to print or share.
The new AHA/ACC guideline: Jones DW, Ferdinand KC, Taler SJ, et al. 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2025 Aug 14. doi: 10.1161/CIR.0000000000001356.
Blumenthal JA, Hinderliter AL, Smith PJ, et al. Effects of Lifestyle Modification on Patients With Resistant Hypertension: Results of the TRIUMPH Randomized Clinical Trial. Circulation. 2021 Oct 12;144(15):1212-1226. doi: 10.1161/CIRCULATIONAHA.121.055329.
Charchar FJ, Prestes PR, Mills C, et al. Lifestyle management of hypertension: International Society of Hypertension position paper endorsed by the World Hypertension League and European Society of Hypertension. J Hypertens. 2024 Jan 1;42(1):23-49. doi: 10.1097/HJH.0000000000003563.
Haghighatdoost F, Hajihashemi P, de Sousa Romeiro AM, et al. Coffee Consumption and Risk of Hypertension in Adults: Systematic Review and Meta-Analysis. Nutrients. 2023 Jul 7;15(13):3060. doi: 10.3390/nu15133060.
Huang L, Trieu K, Yoshimura S, et al. Effect of dose and duration of reduction in dietary sodium on blood pressure levels: systematic review and meta-analysis of randomised trials. BMJ. 2020;368:m315. doi:10.1136/bmj.m315
Hinderliter AL, Smith P, Sherwood A, Blumenthal J. Lifestyle Interventions Reduce the Need for Guideline-Directed Antihypertensive Medication. Am J Hypertens. 2021 Oct 27;34(10):1100-1107. doi: 10.1093/ajh/hpab090.
Juraschek SP, Miller ER, Weaver CM, Appel LJ. Effects of Sodium Reduction and the DASH Diet in Relation to Baseline Blood Pressure. J Amer College Cardiology. Nov 2017, 24343; DOI:10.1016/j.jacc.2017.10.011
National Academies of Sciences, Engineering, and Medicine. 2019. Dietary Reference Intakes for sodium and potassium. Washington, DC: The National Academies Press. doi: https://doi.org/10.17226/25353. (See Chapter 10 for potassium content discussed here.)
Reynolds AN, Akerman A, Kumar S, et al. Dietary fibre in hypertension and cardiovascular disease management: systematic review and meta-analyses. BMC Med. 2022 Apr 22;20(1):139. doi: 10.1186/s12916-022-02328-x.
Theodoridis X, Chourdakis M, Chrysoula L, et al. Adherence to the DASH Diet and Risk of Hypertension: A Systematic Review and Meta-Analysis. Nutrients. 2023 Jul 24;15(14):3261. doi: 10.3390/nu15143261.
Trevano FQ, Vela-Bernal S, Facchetti R, Cuspidi C, Mancia G, Grassi G. Habitual coffee consumption and office, home, and ambulatory blood pressure: results of a 10-year prospective study. J Hypertens. 2024 Jun 1;42(6):1094-1100. doi: 10.1097/HJH.0000000000003709.
Yang T et al. Hypertension and the Gut Microbiome: A Science Advisory From the American Heart Association. Hypertension. 2025 Sep;82(9):e160-e170. doi: 10.1161/HYP.0000000000000247.
Yin X, Rodgers A, Perkovic A, et al. Effects of salt substitutes on clinical outcomes: a systematic review and meta-analysis. Heart. 2022 Sep 26;108(20):1608-1615. doi: 10.1136/heartjnl-2022-321332. Access via Google Scholar.
Published : September 19, 2025
Tagged: AHA guidelines, DASH diet, healthy diet, healthy eating, healthy lifestyle, heart health, high blood pressure, Hypertension guidelines, potassium
Meet the author/educator

Karen Collins
MS, RDN, CDN, FAND
I Take Nutrition Science From Daunting to Doable.™
As a registered dietitian nutritionist, one of the most frequent complaints I hear from people — including health professionals — is that they are overwhelmed by the volume of sometimes-conflicting nutrition information.
I believe that when you turn nutrition from daunting to doable, you can transform people's lives.
Accurately translating nutrition science takes training, time and practice. Dietitians have the essential training and knowledge, but there’s only so much time in a day. I delight in helping them conquer “nutrition overwhelm” so they can feel capable and confident as they help others thrive.
I'm a speaker, writer, and nutrition consultant ... and I welcome you to share or comment on posts as part of this community!
{kind=link}